Beyond the Operating Table: How Shockwave and Laser Therapy Are Redefining Perioperative Musculoskeletal Care
- Jonathan Hall

- 1 day ago
- 15 min read
Surgery is often framed as a singular event, a defined boundary between injury and recovery. But in musculoskeletal medicine, that framing misses something critical: the biological state of the tissues on either side of that boundary profoundly shapes what happens during it, and what follows.
At Movement Mechanics Osteopathy, we've adopted a different approach. Drawing on osteopathic principles that view the body as an integrated, self-regulating system, we ask a question that doesn't get asked often enough in surgical planning: what can we do to the tissue environment before the procedure, and what can we do in the weeks following to support the body's own capacity to heal?
The answer, supported by a growing body of mechanistic and clinical research, involves two modalities we use daily in our clinic: EMS DolorClast® Extracorporeal Shockwave Therapy (ESWT), both focused and radial, and High-Power Laser Therapy at 905nm. Neither is new in isolation. What is novel is their deliberate, perioperative application: used to create an optimal tissue environment before surgery, and to accelerate the biological healing cascade after it.
This is not yet a formally validated protocol with its own randomised controlled trial. We want to be transparent about that. What it is, however, is a clinically-informed hypothesis built on strong mechanistic evidence, evidence that tells us exactly what these modalities do at a cellular and tissue level, and that strongly suggests those effects are precisely what perioperative tissues need. We present that case here.
The Prehabilitation Evidence Base, Better In, Better Out

The concept of prehabilitation, optimising a patient's physical state before elective surgery, is now well-supported in the literature. Systematic review and meta-analysis data consistently shows that patients who enter surgery in better physical condition experience faster postoperative recovery, fewer complications, and reduced hospital stays (Talen et al., 2025).
A 2024 systematic review and meta-analysis examining prehabilitation in frail and high-risk surgical patients confirmed that multimodal preoperative interventions meaningfully reduced postoperative complications and length of stay (Carli et al., 2024). In orthopaedic populations specifically, a 2023 systematic review of 48 unique trials involving 3,570 participants found level I moderate-certainty evidence supporting prehabilitation's impact on surgical outcomes.
The mechanism is straightforward: pre-surgical function is a robust predictor of post-surgical function. What is explored far less, and where our clinical interest lies, is whether the biological preparation of the specific tissues being operated on can augment that effect further. Not just conditioning the cardiovascular system or quadriceps strength, but optimising the vascular supply, collagen architecture, and cellular metabolic state of the operative target itself.
This is the gap we are working in. And the evidence for what shockwave therapy and laser therapy do to tissues at a biological level gives us strong reason to believe they belong in that gap.

What Shockwave Therapy Does to Tissue, The Mechanistic Case

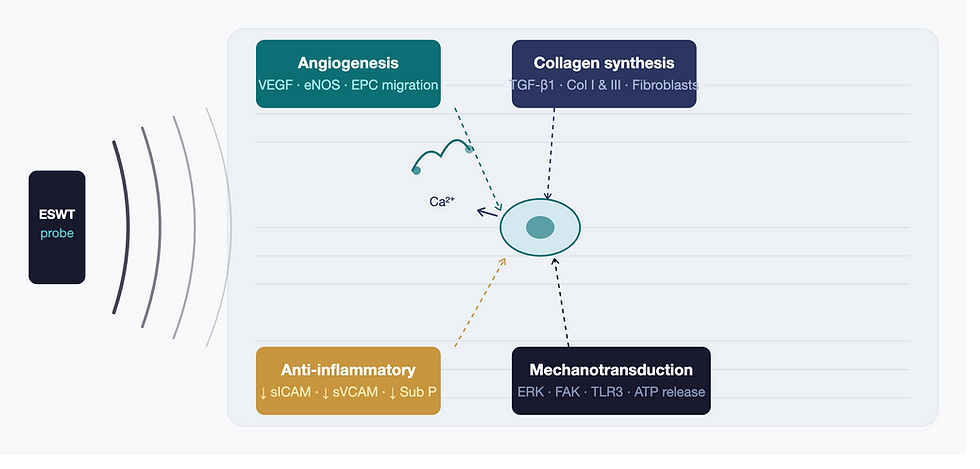
Extracorporeal Shockwave Therapy works through a process called mechanotransduction, the conversion of mechanical force into intracellular biochemical signals. When acoustic waves are delivered to tissue, they activate mechanosensory complexes including ion channels, integrins, and cytoplasmic proteins, triggering downstream gene expression changes that drive tissue remodelling and repair (Ryskalin et al., 2025).
The biological effects of ESWT that are most relevant to perioperative care include:
Angiogenesis: ESWT stimulates upregulation of VEGF (vascular endothelial growth factor), eNOS (endothelial nitric oxide synthase), and endothelial progenitor cell (EPC) migration, promoting new blood vessel formation in previously hypovascular tissue (Liu et al., 2022). This is one of the most consistently replicated findings across the ESWT literature.
Collagen synthesis and ECM remodelling: Shockwave treatment enhances fibroblast proliferation and differentiation through activation of TGF-β1 gene expression and upregulation of Collagen Types I and III, the primary structural collagens in tendons, ligaments, and periarticular soft tissue (Revenaugh, as cited in PMC 2013).
Anti-inflammatory modulation: ESWT reduces concentrations of pro-inflammatory mediators including sICAM-1 and sVCAM-1, and has been shown to shift the local tissue environment from chronic inflammation toward a regenerative state (Zwiauer et al., 2025).
Anti-fibrotic effects: Both focused and radial ESWT demonstrate anti-fibrotic properties through suppression of fibrotic signalling pathways, softening tissue densification and reducing scar formation, critically relevant post-operatively (Zwiauer et al., 2025).
Osteogenic stimulation: Focused ESWT stimulates osteoblast activity and bone morphogenetic protein (BMP) expression, supporting bone consolidation and healing, relevant for any surgical procedure involving bone (Ryskalin et al., 2025).
Pain modulation: ESWT influences substance P release and free nerve ending activity, producing measurable analgesic effects that reduce pre-operative pain burden and post-operative pain sensitisation (Schmitz et al., 2015).
These are not theoretical effects. They are documented in preclinical models and increasingly in clinical populations across a wide range of musculoskeletal conditions. A 2025 perspective synthesising evidence from 2020–2025 across ESWT trials reported GRADE B–A– level evidence for mechanotransduction, angiogenesis, and ECM remodelling effects, supporting moderate-to-high clinical certainty (Ezzati et al., 2020).
Focused vs. Radial ESWT - Two Tools, Complementary Roles
The EMS DolorClast® platform delivers both focused and radial shockwave, and understanding the distinction matters clinically, particularly in perioperative planning.
Featue | Focused ESWT (fESWT) | Radial ESWT (rESWT) |
Wave Type | True shockwave - positive and negative pressure phases | Pressure wave - positive phase only |
Tissue Depth | Up to 12cm - targets deep structures | Superficial - 0–3cm from applicator |
Energy Delivery | Convergent - precise focal zone | Divergent - broader treatment area |
Best Pre-op Use | Deep tendon remodelling, bone perfusion, deep calcific deposits | Fascial preparation, trigger point release, superficial tissue |
Best Post-op use | Deep wound healing support, bone consolidation | Scar tissue management, superficial soft tissue healing |
In practice, focused ESWT lets us target the exact structure being operated on, a degenerating rotator cuff, an Achilles tendon, a tibial non-union, with precision. Radial ESWT allows us to treat the broader soft tissue environment: the surrounding musculature, fascial planes, and compensatory tissue changes that have developed around the primary pathology. Together, they mirror the osteopathic approach to care, addressing both the focal pathology and the wider tissue context.
What High-Power Laser Therapy Does at a Cellular Level

Photobiomodulation (PBM) using pulsed 905nm laser technology operates within the near-infrared therapeutic window, the range of wavelengths at which light achieves maximal penetration into biological tissue with minimal energy loss from absorption and scattering.
The primary mechanism is mitochondrial. Near-infrared light is absorbed by cytochrome c oxidase (CCO), the terminal enzyme of the mitochondrial electron transport chain. This absorption upregulates CCO activity, releasing inhibitory nitric oxide from the enzyme complex and restoring electron transport efficiency. The downstream effects include:
Increased cellular ATP production, meeting the high energy demands of tissue repair
Generation of controlled reactive oxygen species (ROS), which activate redox-sensitive transcription factors driving cellular proliferation and differentiation
Elevated intracellular calcium signalling, activating growth factor synthesis and anti-inflammatory gene expression
Nitric oxide release, promoting vasodilation, angiogenesis, and protection from oxidative damage (Hamblin, 2018)
At a tissue level, these cellular effects translate into fibroblast activation, increased collagen and hyaluronic acid synthesis, enhanced DNA repair capacity, upregulation of VEGF and FGF2 (Fibroblast Growth Factor 2), and modulation of inflammatory mediators including IL-6 and TNF-α (Maghfour et al., 2024). Red and near-infrared wavelengths have demonstrated stimulatory effects on fibroblast cell lines, leading to metabolic activation and increasing the synthesis of collagen, elastin, and hyaluronic acid (Frontiers in Photonics, 2024).
The 905nm superpulsed delivery used by the EMS DolorClast® laser system is particularly relevant for musculoskeletal applications. High peak power delivered in ultra-short pulses allows significant photonic energy to reach deep tissue structures, tendons, joint capsules, peri-osseous tissues, without thermal accumulation, making it both effective and safe for use around post-surgical sites.
It is worth noting that while the biological mechanisms of photobiomodulation are well-established, the literature at 905nm specifically is extrapolated in part from adjacent wavelengths (810nm, 830nm) where the evidence base is most developed. The EMS DolorClast® 905nm system's high peak power delivery distinguishes it from lower-powered systems studied in earlier trials, and clinical outcomes with this system reflect that difference.
The Pre-Operative Application - Preparing the Biological Environment

Conventional surgical planning addresses systemic preparation: cardiovascular optimisation, nutritional status, medication management. What is rarely targeted is the local biological state of the tissue being operated on. We believe this is a missed opportunity, and the mechanistic case for addressing it is compelling.
1. Improving vascularity before the incision
Surgical healing is fundamentally an angiogenic process. Tissues with better baseline vascularity deliver more oxygen, growth factors, and repair cells to the healing site from the moment surgery concludes. The problem is that many of the structures that require surgical intervention, chronically degenerated tendons, calcific deposits, avascular fibrocartilage, are precisely the tissues with the poorest vascular supply.
Pre-operative ESWT's documented capacity to upregulate VEGF and drive endothelial progenitor cell migration means that in the 3–6 weeks before surgery, we can work to improve the capillary network surrounding the operative target. If we can shift tissue from hypovascular to better-perfused before a knife is picked up, the healing response that surgery initiates has better raw materials to work with.
2. Remodelling degenerated extracellular matrix
Degenerated musculoskeletal tissue, rotator cuff tendons, Achilles tendons, calcified structures, exhibits disorganised collagen architecture, increased proteoglycan ground substance, and fibrotic change. It is more difficult to work with surgically, and carries greater risk of re-tear and failure.
The combination of ESWT's TGF-β1-mediated collagen remodelling and laser therapy's fibroblast activation and hyaluronic acid upregulation can begin the process of ECM normalisation before surgery. A 4–6 week pre-operative protocol may meaningfully shift the target tissue from a degenerative to a transitionally reparative state, better organised, better hydrated, and more biologically ready for the acute repair phase that surgery initiates.
3. Reducing chronic inflammatory load
Many surgical candidates have been living with chronic inflammation in the target tissue for months or years. This creates a hostile environment for healing, one characterised by elevated pro-inflammatory cytokines, sensitised nociceptors, and suppression of the regenerative signals needed for tissue repair. Pre-operative modulation of IL-6, TNF-α, sICAM-1, and prostaglandins, effects demonstrated by both ESWT and laser therapy, may shift the tissue microenvironment toward a state more conducive to post-surgical healing.
4. Pre-operative pain management
Pre-operative pain level is a well-established predictor of post-operative pain experience, analgesic requirements, and recovery trajectory. The analgesic effects of both ESWT and laser therapy, operating through substance P modulation, nociceptor desensitisation, and prostaglandin E2 reduction, provide meaningful clinical value independent of their tissue-level effects. Patients who approach surgery with lower pain, less central sensitisation, and improved tissue mobility are better positioned for the perioperative experience.
5. Bone preparation for orthopaedic procedures
For procedures involving bone, total joint replacement, corrective osteotomy, fixation of non-union, focused ESWT has documented osteogenic effects via BMP stimulation and osteoblast activation. Clinical studies have reported radiographic and symptom outcomes after high-energy focused ESWT in humeral delayed union and non-union cases (Ryskalin et al., 2025). Priming bone metabolism before planned orthopaedic surgery represents a hypothesis directly supported by this evidence.
The Post-Operative Application - Accelerating the Healing Cascade

Surgery creates a controlled, targeted biological trauma. The healing response that follows, haemostasis, inflammation, proliferation, remodelling, is precisely orchestrated. The goal of post-operative modality treatment is not to override this process, but to support and accelerate it without disrupting its architecture.
Early post-operative phase (Days 1–5): Laser therapy begins
High-power laser therapy can be applied safely from the first days post-surgery, once the wound is closed, with treatment targeting the peri-operative tissue rather than the wound itself. At this stage, its primary value is in anti-inflammatory modulation, suppressing excess IL-6 and TNF-α while preserving the pro-inflammatory signals that are essential for initiating healing. Simultaneously, laser's stimulation of mitochondrial ATP production supports the high energy demands of the initial repair response.
Proliferative phase (Days 5–21): Where laser therapy excels
This is the phase of fibroblast activation, collagen deposition, and angiogenesis, exactly the biological processes that photobiomodulation is most effective at supporting. Laser therapy's documented stimulation of fibroblast proliferation, TGF-β1 expression, VEGF upregulation, collagen synthesis, and DNA repair places it as a highly logical adjunct during this window. A 2024 narrative review of high-intensity laser therapy's efficacy in wound healing found supporting evidence across multiple clinical contexts (Yoon et al., 2024). Every session during this phase is potentially catalysing earlier and higher-quality tissue deposition.
Remodelling phase (Weeks 3–12+): Shockwave is introduced
Once the tissue has sufficient structural integrity to tolerate mechanical stimulation, radial ESWT can be introduced to address scar tissue formation, promote collagen fibre maturation, and prevent excessive fibrosis, one of the most common complications following tendon repair, joint reconstruction, and spinal surgery. The anti-fibrotic capacity of ESWT is well-documented in the literature (Ryskalin et al., 2025). Focused ESWT can be added for deeper scar remodelling and bone consolidation where indicated.
Return to function (Months 3–6+): Combined protocols
As patients progress into active rehabilitation, integrated shockwave and laser protocols support tissue maturation, address residual pain foci, and optimise the final architecture of the healing tissue. This is also where the osteopathic dimension of our work becomes most important, manual therapy, movement re-education, and addressing the compensatory patterns that have developed over months or years of dysfunction.
The Osteopathic Framework, Why We Don't Just Treat the Target Tissue

The application of shockwave and laser therapy at Movement Mechanics Osteopathy does not happen in isolation from a broader clinical framework. Osteopathic medicine holds as a core principle that structure and function are reciprocally interrelated, and that the health of any tissue cannot be understood apart from the system that supplies, moves, and loads it.
A degenerating Achilles tendon awaiting surgical repair exists within a kinetic chain characterised by altered ankle dorsiflexion, reduced calf extensibility, hip abductor weakness, compensatory lumbar loading, and nervous system sensitisation. Effective perioperative care must address this chain, not just the target tissue.
Our perioperative framework therefore integrates:
Targeted modality application - focused ESWT and/or high-power laser to the operative tissue, selected based on depth, pathology type, and phase of care
Osteopathic manual therapy - addressing somatic dysfunction, joint mobility, fascial restriction, and neural tension in the broader kinetic chain
Radial ESWT for surrounding soft tissue - treating the musculature, trigger points, and fascial adherences that have developed as compensatory responses to the primary pathology
Progressive movement rehabilitation - guided return to function integrating neuromuscular re-education and tissue loading progression appropriate to the surgical timeline
Patient education and surgical preparation - ensuring patients understand what to expect, how to support their own recovery, and what the post-operative rehabilitation pathway looks like before they arrive in theatre
This is what we mean by a holistic approach to surgical care. Not an alternative to surgery, in many cases surgery is the right decision and we fully support it, but a commitment to ensuring the body is as well-prepared as possible to go through it, and as well-supported as possible to recover from it.
Conditions We Commonly Manage Perioperatively
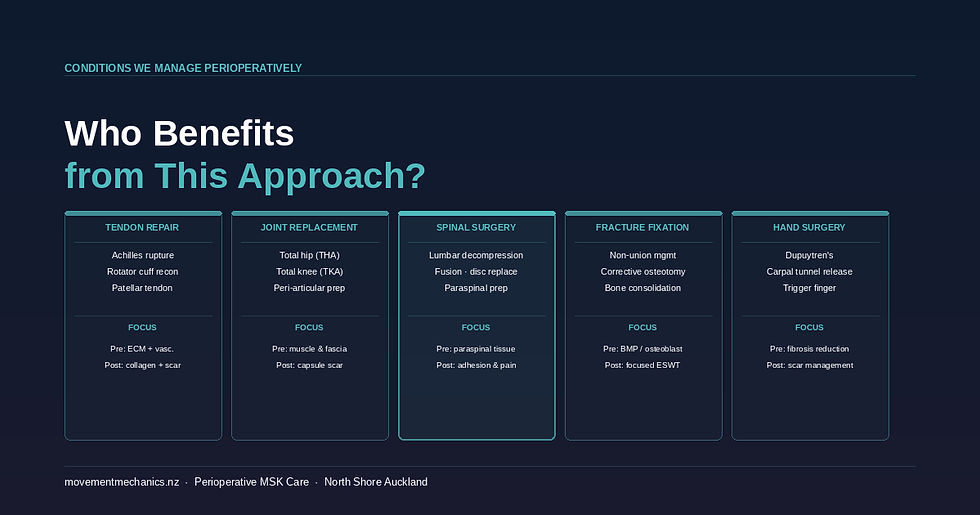
Tendon repair surgery
Achilles tendon rupture repair, rotator cuff reconstruction, and patellar tendon repair represent some of the most common surgical procedures in our patient population. These tendons, particularly in the degenerative state that precedes surgical failure, exhibit exactly the biology that ESWT and laser address: poor vascularity, disorganised collagen, elevated inflammatory mediators, and compromised fibroblast activity. Pre-operative preparation and post-operative acceleration of healing represent the clearest application of our model.
Total joint replacement
The peri-articular soft tissue environment at the time of total hip or knee arthroplasty significantly influences rehabilitation. Pre-operative laser and radial ESWT to the periarticular musculature, and post-operative protocols addressing scar capsule formation, quadriceps inhibition, and pain are meaningful additions to standard physiotherapy prehabilitation.
Spinal surgery
Lumbar decompression, fusion, and disc replacement are performed in a tissue environment, the paraspinal musculature, facet joints, and posterior ligament complex, that is frequently degenerated, deconditioned, and hypovascularised. Pre-operative laser and ESWT to the lumbar tissues, and post-operative management of paraspinal scar, adhesion, and pain, may meaningfully influence recovery speed and quality.
Fracture fixation and non-union
Focused ESWT has arguably its most mature evidence base in bone healing indications. For patients with delayed unions or planned corrective osteotomies, pre-operative focused ESWT may prime the bony environment for consolidation. Post-operatively, it supports non-invasive adjunctive bone healing alongside the fixation the surgery has created.
Hand and wrist surgery
Systematic review evidence has identified both ESWT and laser therapy among the pre-operative hand therapy interventions studied for Dupuytren's disease and related conditions, reflecting growing interest in perioperative modality application in hand surgical populations (PMC, 2024).
Our Clinical Hypothesis - Where We Stand on the Evidence
We want to be clear about what we know and what we are proposing. The individual biological effects of ESWT and photobiomodulation at 905nm are well-established in the literature, mechanotransduction, angiogenesis, collagen synthesis, anti-inflammatory modulation, ATP upregulation, fibroblast activation. The clinical evidence for these modalities in treating established musculoskeletal pathology is robust across multiple conditions and levels of evidence.
What is novel is their deliberate, protocol-driven application specifically as perioperative tissue preparation and healing augmentation tools within an osteopathic framework. This represents a clinically-informed hypothesis, not yet a validated perioperative protocol in its own right.
The hypothesis: Pre-operative biological tissue preparation using ESWT and laser therapy, by improving vascularity, ECM organisation, cellular metabolic state, and inflammatory balance of the operative target, may reduce surgical difficulty, improve repair site quality, accelerate the post-operative healing cascade, reduce complication rates, and produce better functional outcomes compared to standard prehabilitation alone. This hypothesis is grounded in established mechanistic biology and the prehabilitation literature demonstrating that better pre-surgical tissue state predicts better outcomes.
What we observe clinically is consistent with this hypothesis: patients who undergo our perioperative protocols appear to enter surgery with better tissue quality (as reported by surgical colleagues), move through the proliferative phase faster, require less analgesic support post-operatively, and achieve rehabilitation milestones earlier. These are clinical observations, not controlled data, but they align with the mechanistic picture the literature presents.
We actively welcome collaboration with surgical teams to design prospective investigation of this approach. The biology justifies formal study.
A Note on Safety and Surgical Coordination
All perioperative protocols at Movement Mechanics Osteopathy are developed in direct consultation with the patient's surgical team. Pre-operative treatment typically concludes 1–2 weeks before surgery. In the immediate post-operative period, laser therapy avoids direct application over active wounds. Radial and focused ESWT are introduced progressively as wound integrity and tissue tolerance allow. Specific timing and contraindication screening are always determined collaboratively with the treating surgeon, and patient safety is non-negotiable in every decision we make.
Frequently Asked Questions
Can shockwave therapy be used before surgery?
Yes. EMS DolorClast® Focused and Radial Shockwave Therapy can be used in the weeks before musculoskeletal surgery to improve tissue vascularity, remodel the extracellular matrix, reduce chronic inflammation, and optimise the biological environment of the operative target. This is a novel perioperative framework developed at Movement Mechanics Osteopathy, grounded in the well-established mechanistic biology of ESWT.
What does laser therapy do after surgery?
High-power laser therapy at 905nm stimulates cytochrome c oxidase in mitochondria, increasing cellular ATP production, reducing IL-6 and TNF-α, upregulating collagen synthesis, and promoting angiogenesis via nitric oxide and VEGF pathways. Post-operatively, these effects accelerate both the proliferative and remodelling phases of tissue healing, and provide non-pharmaceutical analgesia during recovery.
How soon after surgery can laser therapy begin?
High-power laser therapy can typically commence once the surgical wound is closed, often within the first few days post-operatively, targeting peri-operative tissue rather than the wound site directly. The exact timing is always determined in consultation with the treating surgeon and tailored to the individual procedure.
What is the difference between focused and radial shockwave therapy for surgical patients?
Focused ESWT delivers high-energy acoustic waves to a precise deep focal point up to 12cm, making it ideal for deep tendons, bone, and calcific deposits. Radial ESWT delivers divergent pressure waves superficially at 0–3cm, better suited for fascial treatment, trigger point release, and post-operative scar remodelling. Both are available via the EMS DolorClast® system and are used at different stages of our perioperative protocols.
What conditions benefit most from perioperative shockwave and laser therapy?
Conditions where perioperative ESWT and laser therapy are most clinically relevant include Achilles tendon and rotator cuff repair surgery, total hip and knee arthroplasty, lumbar spine procedures, fracture fixation and non-union management, and hand surgery for conditions such as Dupuytren's contracture. The common thread is the presence of degenerated, hypovascular, or chronically inflamed tissue that can benefit from biological preparation before surgical intervention.
Does osteopathy play a role in perioperative care?
Absolutely. The osteopathic framework, addressing the whole kinetic chain, not just the target tissue, is central to how we approach perioperative management at Movement Mechanics. Manual therapy, movement re-education, and compensation pattern management are integrated alongside shockwave and laser therapy in our perioperative protocols, ensuring that tissue-level improvements are supported by functional and structural changes across the broader system.
Where can I access perioperative shockwave and laser therapy on Auckland's North Shore?
Movement Mechanics Osteopathy offers EMS DolorClast® Focused and Radial Shockwave Therapy and High-Power Laser Therapy at our clinic in Browns Bay, 13–15 Bute Road. We provide same-week appointments, ACC support, and integrated perioperative treatment plans tailored to your specific procedure and tissue.
Jonathan Hall M.Ost, BAppSci (Human Biology), PGCertHSc (Acupuncture), GradDipHeal, FIFA Diploma in Football Medicine
Jonathan Hall is the founder and principal Osteopath at Movement Mechanics Osteopathy. Jonathan specialises in Shockwave Therapy and Western Medical Acupuncture and is a Key Opinion Leader for EMS Swiss DolorClast. A fully qualified Osteopath registered with OCNZ, PNZ, PAANZ and ACC, Jonathan also founded Auckland Shockwave Therapy to bring evidence-based shockwave treatment to New Zealand using the industry-leading EMS DolorClast® device.
Contact Us: hello@movementmechanics.nz
References
Carli, F., Bousquet-Dion, G., Awasthi, R., Elsherbini, N., Liberman, S., Boutros, M., Stein, B., & Feldman, L. (2024). The impact of prehabilitation on outcomes in frail and high-risk patients undergoing major abdominal surgery: A systematic review and meta-analysis. Clinical Nutrition. https://doi.org/10.1016/j.clnu.2024.01.012
d'Agostino, M. C., Craig, K., Tibalt, E., & Respizzi, S. (2015). Shock wave as biological therapeutic tool: From mechanical stimulation to recovery and healing, through mechanotransduction. International Journal of Surgery, 24(Pt B), 147–153. https://doi.org/10.1016/j.ijsu.2015.11.030
Ezzati, K., Laakso, E.-L., Salari, A., Hasannejad, A., Fekrazad, R., & Aris, A. (2020). The beneficial effects of high-intensity laser therapy and co-interventions on musculoskeletal pain management: A systematic review. Journal of Lasers in Medical Sciences, 11(1), 81–90. https://doi.org/10.15171/jlms.2020.14
Hamblin, M. R. (2018). Mechanisms and mitochondrial redox signalling in photobiomodulation. Photochemistry and Photobiology, 94(2), 199–212. https://doi.org/10.1111/php.12864
Liu, J., Chen, L., Liu, J., Wang, Y., & Guo, Y. (2022). Biological response of extracorporeal shock wave therapy to tendinopathy in vivo. Frontiers in Veterinary Science, 9, 851894. https://doi.org/10.3389/fvets.2022.851894
Maghfour, J., Ozog, D. M., Mineroff, J., Jagdeo, J., Kohli, I., & Lim, H. W. (2024). Photobiomodulation CME part I: Overview and mechanism of action. Journal of the American Academy of Dermatology, 91(4), 793–802. https://doi.org/10.1016/j.jaad.2023.10.073
Ryskalin, L., Fulceri, F., D'Agostino, M. C., Vetrano, M., Vulpiani, M. C., & Gesi, M. (2025). Recent advances in shockwave therapy for musculoskeletal and soft-tissue disorders. Life, 15(12), 1912. https://doi.org/10.3390/life15121912
Schmitz, C., Császár, N. B. M., Milz, S., Schieker, M., Maffulli, N., Rompe, J. D., & Furia, J. P. (2015). Efficacy and safety of extracorporeal shock wave therapy for orthopedic conditions. British Medical Bulletin, 116, 115–138. https://doi.org/10.1093/bmb/ldv047
Talen, A. D., van Meeteren, N. L. U., Barten, J. A., Pereboom, I., Krijnen, W. P., Jager-Wittenaar, H., Bongers, B. C., & van der Sluis, G. (2025). The challenges of evidence-based prehabilitation in a real-life context for patients preparing for colorectal surgery: A cohort study and multiple case analysis. Perioperative Medicine, 14, Article 3. https://doi.org/10.1186/s13741-024-00481-w
Yoon, S. H., Huh, B. K., Abdi, S., & Javed, S. (2024). The efficacy of high-intensity laser therapy in wound healing: A narrative review. Lasers in Medical Science. https://doi.org/10.1007/s10103-024-04146-4
Zwiauer, S., Urban, N., & Schmitz, C. (2025). Penetration depth and tissue interaction of focused extracorporeal shock waves: An in-vitro investigation. Cureus, 17(3), e81234. https://doi.org/10.7759/cureus.81234
Disclaimer: This content is for educational purposes and does not constitute medical advice. Individual patient suitability for perioperative shockwave and laser therapy should be assessed by a qualified healthcare practitioner in direct collaboration with the treating surgical team. Contraindications to ESWT and photobiomodulation must be screened for prior to treatment.

Comments